
Two Machines, One Question: What Tesofensine’s Chemistry Actually Tells Us About the “Stronger Than Ozempic” Claim

Ask a chemist to explain why a stimulant and a hormone can both make someone lose weight, and the answer usually takes longer than the question. That is more or less the situation with tesofensine and the GLP-1 drugs. People keep asking which one is “stronger,” as if the two were different horsepower ratings on the same engine. They are not the same engine. One runs on gut hormones. The other runs on brain chemistry that has nothing to do with the gut at all. Before any comparison can mean anything, it helps to understand what each drug is actually doing inside the body, because the mechanisms explain almost everything that follows, including why the evidence for one is so much thinner than the evidence for the other.
The biology, plainly
Semaglutide and tirzepatide are peptides, chains of amino acids built to resemble a hormone the gut releases after eating. Injected under the skin, they latch onto the GLP-1 receptor (tirzepatide also hits the GIP receptor) and, through that hormonal signaling, slow stomach emptying, dial up fullness, and quiet appetite circuits in the brain. It is a metabolic mechanism, discovered and engineered on purpose, and it now has an FDA approval and a stack of large modern trials behind it.
Tesofensine works through an entirely different door. It is a small molecule, first labeled NS2330, taken as a pill, and it belongs to a drug class called triple monoamine reuptake inhibitors. In plain terms: after serotonin, norepinephrine, and dopamine get released in the brain’s synapses, the brain normally vacuums a portion of them back up. Tesofensine blocks that vacuum on all three neurotransmitters at once, so they linger longer where they were released. That is the same broad mechanical family as certain antidepressants and stimulants, not the gut-hormone family. It is also, in the United States, still an investigational compound rather than an approved drug.
So the question “is tesofensine stronger than Ozempic” is really asking whether a brain-chemistry pill outperforms a gut-hormone injection, two different biological systems that were never built to be measured against each other on the same scale. That mismatch is the whole reason the question resists a clean answer.
Where the number actually comes from
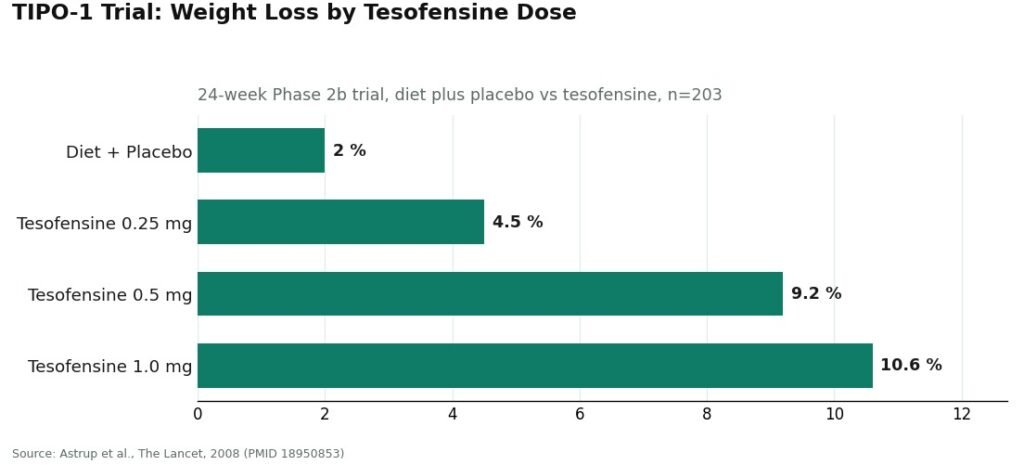
The claim has a specific origin, and it is worth tracing to its source rather than taking on faith. It comes from one trial: TIPO-1, a Phase 2b study published in The Lancet in 2008. Researchers ran it properly, randomized, double-blind, placebo-controlled, across five Danish obesity centers, 203 patients with a BMI of 30 to 40, all following a calorie-restricted diet, for 24 weeks. Diet plus placebo produced 2.0% weight loss. Diet plus tesofensine produced 4.5% at 0.25 mg, 9.2% at 0.5 mg, and 10.6% at 1.0 mg [P1].
That is a real dose-response curve, and a notable one for a mid-stage trial. The authors themselves wrote that the 0.5 mg dose “might have the potential to produce a weight loss twice that of currently approved drugs” [P1]. That single sentence is the entire basis for every “stronger than Ozempic” headline that followed. But the same sentence continues, in the same paper, that the finding “needs confirmation in phase III trials” [P1]. That second half rarely makes it into the headline.
Three details matter here for anyone trying to read the number honestly. The comparator drugs in that 2008 sentence were the weight-loss drugs available in 2008, a much weaker shelf than what semaglutide and tirzepatide represent today. The placebo arm already produced 2.0% loss on its own, so the effect attributable to the drug itself is closer to 7.2% at 0.5 mg and 8.6% at 1.0 mg, a real number but not the double-digit figure people quote [P1]. And it was Phase 2, a stage explicitly meant to be followed by a larger confirmatory trial. Seventeen years later, that confirmatory Phase 3 program has not produced a US approval.
The comparison that has never actually happened
Here is the detail that resolves the “which is stronger” question more than any other: no trial has ever put tesofensine and a GLP-1 drug in the same room. Every claim ranking them draws from separate studies, run in different years, on different populations, under different protocols, then lined up after the fact. That kind of cross-trial comparison is a known source of error in clinical research, because differences in patient selection, trial length, and background diet can swing the numbers as much as the drug itself does. A real answer would require a head-to-head randomized trial. That trial does not exist. Until it does, “stronger” is an inference, not a finding.
What the timeline actually shows, once you line it up
Set the ranking question aside for a moment and look at the calendar instead, because the gap in evidence age turns out to be more informative than the gap in percentages.
The GLP-1 case rests on an evidence base that keeps being renewed: repeated, large, recent randomized trials, an FDA approval sitting on top of them. The tesofensine case rests on a single strong data point frozen in 2008, plus supporting mechanistic work (imaging studies showing dose-dependent dopamine transporter occupancy up to about 77% [P3], and rodent studies pointing to alpha-1 adrenoceptor and dopamine D1 receptor pathways as the likely drivers of the appetite effect [P4]), but no completed US Phase 3 in the years since. As of the public record in mid-2026, tesofensine’s furthest regulatory step anywhere is a favorable technical-committee opinion from Mexico’s COFEPRIS in early 2023, a procedural note, not an approval. One evidence base is a photograph from 2008. The other is closer to a video still being filmed.
That gap also shows up in what got studied on the cardiovascular side. In TIPO-1, heart rate rose about 7.4 bpm at the 0.5 mg dose [P1]. An earlier 2008 meta-analysis of tesofensine’s original Parkinson’s and Alzheimer’s trials found the same pattern even without dieting, up to roughly 6.8 bpm, dose-dependently [P2]. The 1.0 mg dose also raised blood pressure enough that it was dropped from later development. The developers took the heart-rate problem seriously enough to run a dedicated Phase 1 study, NCT03488719, pairing tesofensine with the beta blocker metoprolol specifically to blunt the effect. The study’s own documentation called heart rate “the most affected safety endpoint” of the drug, and the trial was halted over safety concerns before ending in 2019 [P5]. That is not a footnote. It is a specific, quantified cost that sits on tesofensine’s side of the ledger and has no real counterpart in the GLP-1 literature.
There is a second cost worth naming plainly, because it is mechanistic rather than incidental: tesofensine raises serotonin along with dopamine and norepinephrine, which means it interacts badly with other serotonergic drugs. Combined with an MAOI, the risk is serotonin syndrome and a hypertensive crisis. It also stacks poorly with SSRIs, SNRIs, stimulants, and bupropion, drugs that a large share of the population already takes. And because the original obesity trials excluded people with known psychiatric conditions, the published record says relatively little about how the compound behaves in minds already managing depression or anxiety. That is an evidence gap, not a clean bill of health.
An accident and an engineering project
It is worth noting how differently these two drug lines began, because it explains some of the asymmetry above. The GLP-1 drugs were designed from the start as metabolic medicines, aimed deliberately at the gut-hormone system. Tesofensine was not designed for obesity at all. The Danish firm NeuroSearch developed it hoping it would help Parkinson’s or Alzheimer’s disease, and it did not work well enough for either. What kept showing up in those trials was weight loss, especially in heavier patients, and the obesity program was built afterward, around a side effect that had been observed rather than targeted. A 2008 meta-analysis of those original neurological trials quantified it: roughly 4% placebo-subtracted weight loss over 14 weeks, with no diet program attached, and that same dose-dependent heart-rate increase [P2]. A drug discovered by accident can still be useful. But it is a different kind of useful than a drug engineered on purpose, and the difference in how thoroughly each has been vetted for obesity specifically traces back to that origin story.
The honest bottom line
Tesofensine and the GLP-1 drugs are not two points on the same scale. One is an approved, hormonally targeted peptide backed by a large and current trial record. The other is an investigational, orally dosed compound with a genuinely different brain mechanism, one strong but aging Phase 2 result, a documented heart-rate effect serious enough to have ended its own countermeasure trial, and a drug-interaction profile that touches some of the most commonly prescribed medications in the country. Reasonable people, working with a clinician, might still choose to explore tesofensine, particularly if the gut-hormone pathway has not worked for them. What is not reasonable is choosing it because a 2008 sentence about “twice the weight loss” got stripped of its context and turned into a slogan.
Given the specific risks here, cardiovascular and pharmacological rather than general, the gap between a supervised path and an unsupervised one matters more than it would for a lower-risk supplement. A telehealth provider like FormBlends operates as a licensed clinical service: a clinician takes a history, records a baseline heart rate and blood pressure, checks current medications against the serotonergic interaction list, and monitors over time, with tesofensine, where available in the US, dispensed as a compounded medication through a licensed 503A pharmacy under prescription. Because it is a small molecule rather than a peptide, it falls outside the FDA’s peptide-compounding restrictions and remains available through that route. HealthRX (healthrx.com) sits in the same supervised tier, for the same reason: oversight is the point, not an afterthought.
The alternative is the research-chemical market, where tesofensine is sold labeled “for research use only, not for human consumption,” language that exists specifically so the seller avoids marketing an unapproved drug for human use. On a compound with a measured heart-rate effect and a real interaction risk with everyday psychiatric medications, that route means no baseline reading, no medication check, and no one to call if something changes. Those are exactly the safeguards this particular drug’s chemistry says are needed.
Questions people actually ask
Is tesofensine stronger than Ozempic? The question can’t really be answered as asked, because the two drugs have never been tested against each other and belong to different pharmacological families altogether, a hormonal injectable peptide against an investigational oral monoamine reuptake inhibitor. The “stronger” claim traces to one 2008 Phase 2 trial that compared itself to the weight-loss drugs available in 2008, not to modern GLP-1 agents. No head-to-head trial exists, so any ranking is an inference across separate studies, not a measured result.
Where does the “twice the weight loss” line come from? From the TIPO-1 Phase 2b trial, published in The Lancet in 2008, where the authors wrote that the 0.5 mg dose “might have the potential to produce a weight loss twice that of currently approved drugs,” a comparison made against 2008-era drugs. The same sentence added that the finding “needs confirmation in phase III trials.” Subtract the 2.0% that diet plus placebo achieved alone, and the drug’s own contribution comes closer to 7.2% at 0.5 mg, not a clean double-digit figure.
Is tesofensine FDA-approved? No. It remains investigational in the United States for any use. Its furthest regulatory step anywhere is a favorable technical-committee opinion from Mexico’s COFEPRIS in early 2023, a procedural note rather than an approval, and as of mid-2026, by the public record, no country has approved it for obesity. The GLP-1 drugs, by contrast, hold FDA approval built on a large, recent randomized-trial record.
What are the biggest risks with tesofensine compared to the GLP-1 drugs? Cardiovascular effects lead the list: heart rate rose about 7.4 bpm at 0.5 mg in TIPO-1, the 1.0 mg dose raised blood pressure enough to be dropped from development, and a dedicated study pairing tesofensine with a beta blocker to counter the heart-rate rise was halted over safety concerns. The second risk is pharmacological overlap: because it raises serotonin, it interacts dangerously with MAOIs and poorly with SSRIs, SNRIs, stimulants, and bupropion, medications a great many people already take.
Can someone on an antidepressant take tesofensine? That determination belongs to a clinician, not a self-assessment. Tesofensine’s serotonin effect can trigger serotonin syndrome or a hypertensive crisis alongside MAOIs, and it interacts poorly with SSRIs, SNRIs, stimulants, and bupropion. Given how common those prescriptions are, a medication review is a standard part of supervised evaluation, and it is precisely the check that goes missing in the research-chemical market.
How is tesofensine obtained legally and safely in the US? Where available, it reaches patients as a compounded medication through a licensed 503A pharmacy, prescribed after a telehealth clinician reviews history, records baseline heart rate and blood pressure, and checks current medications, with follow-up monitoring afterward. Its status as a small molecule, rather than a peptide, keeps it outside the FDA’s peptide-compounding restrictions. Buying it instead as a “research use only” chemical strips away every one of those checks, on a drug whose specific risks are exactly what those checks are designed to catch.
What is tesofensine and how does it differ from GLP-1 drugs?
Tesofensine blocks the brain’s reabsorption of three neurotransmitters at once, dopamine, serotonin, and norepinephrine, which is what suppresses appetite and appears to nudge up energy expenditure. GLP-1 drugs like semaglutide instead mimic a gut hormone and signal through hormone receptors. The two hit completely different biological targets, which is exactly why ranking one as flatly “stronger” glosses over how differently they actually work.
What is tesofensine used for, and is it approved?
Tesofensine started life as a candidate for Parkinson’s and Alzheimer’s disease. Weight loss showed up as a side effect strong enough that researchers redirected the program toward obesity. It still has no FDA or EMA approval for any use, so it isn’t a legal over-the-counter option in most countries. Outside of clinical trials, access generally runs through a physician-supervised compounding pathway, such as a compounding pharmacy like FormBlends.
Does tesofensine actually burn fat, or does it just reduce appetite?
Both seem to play a role, though appetite suppression looks like the larger factor. Trial data suggest a modest bump in resting metabolic rate as well, which would add to fat loss beyond simply eating less. Researchers haven’t cleanly separated how much each contributes, and the evidence base is still fairly small, so specific claims about fat-burning should be treated cautiously until bigger trials report.
Is tesofensine a peptide like semaglutide or tirzepatide?
No. Tesofensine is a small molecule, not a peptide, which is why it can be taken as a capsule rather than an injection, unlike semaglutide and tirzepatide, which are peptide chains that would break down if swallowed. It acts in the brain rather than through hormone receptors, and that difference in mechanism carries through to a different side-effect profile and different tolerability questions between the two drug types.
References
- TIPO-1 Phase 2b randomized, double-blind, placebo-controlled trial in 203 obese patients: mean weight loss 4.5% / 9.2% / 10.6% at 0.25 / 0.5 / 1.0 mg vs 2.0% placebo over 24 weeks; heart rate +7.4 bpm at 0.5 mg; authors concluded the 0.5 mg result needs Phase 3 confirmation. Astrup et al., The Lancet, 2008. PMID 18950853. https://pubmed.ncbi.nlm.nih.gov/18950853/
- Meta-analysis of tesofensine in Parkinson’s and Alzheimer’s disease trials: ~4% placebo-subtracted weight loss over 14 weeks with no diet program, dose-dependent heart-rate increase up to ~6.8 bpm. Astrup et al., Obesity (Silver Spring), 2008. PMID 18356831. https://pubmed.ncbi.nlm.nih.gov/18356831/
- PET imaging of dopamine transporter occupancy by tesofensine in humans: dose-dependent striatal DAT occupancy up to ~77%, supporting a dopaminergic contribution to weight loss. Appel et al., European Neuropsychopharmacology, 2014. PMID 24239329.
- Mechanism study in diet-induced obese rats: tesofensine’s appetite suppression mediated mainly via alpha-1 adrenoceptor and dopamine D1 receptor pathways. Axel, Mikkelsen, Hansen, Neuropsychopharmacology, 2010. PMID 20200509.
- Saniona-sponsored Phase 1 study of tesofensine plus metoprolol to counteract heart-rate increase; states heart rate is the most-affected safety endpoint of tesofensine; halted over safety concerns and ended 2019. NCT03488719.
- Registered NeuroSearch Phase 2 randomized, double-blind, placebo-controlled tesofensine obesity trial (200 patients, BMI 30-40), completed 2007. NCT00394667.
